
This post concerns several things that have been on my mind for a while.
Photography
During the 2017 end-of-year holidays, I dropped and damaged the mirror box of my Nikon D5100 baby DSLR. It was not a new camera when I bought it on eBay (circa 2012), but it has worked flawlessly for the years I have owned it. Indeed had I not dropped it, it would have yielded at least another five years of service. I was pretty upset when I discovered it was damaged but excited that the attached lens was in good shape. I was also excited at the prospect of buying a new camera. The D5100 was released in April 2011, and in the intervening years, more recent and more capable cameras were introduced by Nikon, Sony, Fuji, Olympus and Canon. Buying a new camera, however, presented a new challenge. Which camera to choose?
There are many buzzes around mirrorless interchangeable lens cameras (MILC). A new term is needed to describe these types of cameras. The term mirrorless camera is as silly as the term horseless carriage. I suggest the time digital viewfinder camera(DVC) or digital interchangeable lens viewfinder(DILV), or electronic viewfinder(EV). Whatever you call it, though, the new style of interchangeable lens camera seems to be popular with many photographers.

Canon EOS 5D Mark III + Canon EF 70-200mm f/2.8L IS II USM @ 70mm ISO 100 1/320s ƒ/4
At one time or another over the last two to three years, I have rented Olympus, Sony, Fuji and Panasonic interchangeable lens cameras. They all have pros and cons, with the newer iterations of each camera improving and reducing the problem areas.
I must look like a wet mangy dog without my camera because my wife's best friend offered to let me use her father's 1 camera and lens, a Canon EOS 5D Mk II with Canon EF 70-200 USM IL f/2.8. The 5D Mk II is a full-frame DSLR with "pro" level features. The EF 70-200 mm lens is worth more than all my existing lenses combined. I've never used Canon cameras and lenses and was trying to figure out what to do with this kit. Last week, after learning from a work colleague that any EF lens will work with the EOS 5D MK II, I started looking for used 35mm and 50mm EF lenses on eBay. Getting a used lens for less than $100 was worth it. I was tired of shooting photos of the birds in the backyard. However, I didn't need to.

I remembered that my Dad had given me his Canon Rebel film camera a few years ago. I knew it was somewhere in the basement. It took a few weeks, but I finally found it. It has a Canon EF 28-80mm f/3.5-5.6 lens. It's compatible with the 5D Mk III. I took the camera and lens on a recent road trip to Michigan and Ohio. I downloaded a few photos and noticed the quality could have been better. The images all seem "hazy". I assumed it was due to poor skill on my part -- shooting images with the light in the background. But I noticed photos taken indoors with front lightning had the same issue. I examined the lens and discovered some semi-transparent "goo" on the inside of the lens.
If I continue to use this lens, I must use the Adobe Lightroom "dehaze" tool for every captured image.
I found some inexpensive Nikon to Canon lens adapters on Amazon. I could use my existing Nikon lenses. The caveat is that the adapters do not allow auto-focus and TTL metering. I promise not to replace my Nikon until after my 2017 taxes are filed. I can't wait. I'll get a deal on a Nikon D500.
I've also struggled with impostor syndrome. I look at the excellent work by an artist like Olaf and. I compare my work to theirs, which is a mistake. Olaf has talent and years of experience. I'm just an amateur who photographs mainly on the weekend. The comparison leaves me feeling inadequate. I put the camera down, and my skills atrophy. Why am I doing this?

Graves Disease
Over 12 years ago, I was diagnosed with Type 1 diabetes. After diagnosis, I started seeing a specialist, an endocrinologist, about every three months. On these regular visits, we discuss my insulin regimen, diet, exercise and the results of my lab tests. The lab results have lots of exciting and helpful information for an endocrinologist, but I only paid attention to the cholesterol and A1C values. But my endo looks at all of it.
One of the things she was testing was my thyroid function, which until recently was normal. And then it wasn't. She tested my thyroid function because people with other immune system diseases, such as type 1 diabetes, have an increased risk of hyperthyroidism. And the onset happened just as rapidly as it did for my Type 1 diabetes. After a battery of tests over a few weeks, my endocrinologist confirmed a diagnosis of Grave's Disease, which the American Thyroid Association describes this way:
Graves' disease, named after Irish physician Robert Graves, is a common cause of hyperthyroidism in the United States. This autoimmune condition leads to the overactivity of the thyroid gland, primarily affecting women (7-8 times more than men).
The disease is triggered by the body's immune system, typically responsible for defending against foreign invaders like bacteria and viruses. However, in Graves' disease, the immune system can produce antibodies that mistakenly target proteins within our own cells. Instead of destroying these cells, these antibodies, known as thyrotropin receptor antibodies (TRAb) or thyroid-stimulating immunoglobulins (TSI), stimulate thyroid cells excessively.
These antibodies bind to receptors on the surface of thyroid cells, prompting them to overproduce and release thyroid hormones. Consequently, this leads to hyperthyroidism, where the thyroid becomes overactive, producing excessive thyroid hormone.

Looking back over the last few months, I know I felt the symptoms of the disease, even though I did know how to interpret them.
I was anxious, irritable, and quite emotional. Anger. And sadness. My hands are shaking slightly, and using a computer -- either a keyboard or touchscreen is more complicated. I am sensitive to heat, and I feel like sweating into my socks. I feel tired while simultaneously feeling energetic (heart palpitations), and falling asleep was challenging. I lost seven pounds.
So now you know. I now have two autoimmune diseases. My endo gave me options for treatment -- pills, surgery, radiation therapy. I opted for the drugs. I am hoping the pills work.
I'll also find out from her what the other results of my lab test mean. Am I at risk for another autoimmune disease?
Work
Work has been stressful since a management change last year. As a consultant, I had worked harmoniously with the previous two managers, but over the last year, I had felt the relationship with the new manager was straining. It was also causing me considerable stress. On Monday, I had a panic attack while at the office. I came home early.
My wife reassured me that she was on board with me leaving. The toxic environment created by this person affected my mental and physical health.

I had started looking for new opportunities elsewhere, but my work for the client ended abruptly this week. I was told that my services were no longer needed. I didn't say a word. I didn't ask why. I said, "OK", packed my day bag, handed in my laptop and pass, and left.
Now, I have time to find my next gig or job. I've spoken to a few recruiters and contacted a few colleagues and friends. Next week, I plan to be busy with interviews and have a few offers by the end of April.
Writing
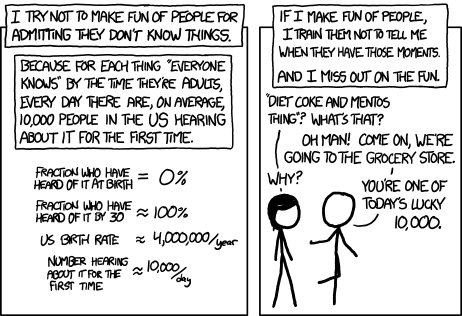
As a blogger, it's easy to fall into the trap of thinking everything I write about is already known by everyone or that my audience on Island on the Net has seen everything I've ever published. It's good to remember that every day, someone might be part of the few to learn something new to them, even if I've written about it previously.
I have a backlog of about 116 articles in draft mode. Most of these are technical articles about photography, web development, and the IndieWeb. I want to set aside time to work on these. Perhaps some will be long-form, but I suspect most will be short.
Diabetes
My diabetes management is reasonably good. I usually keep my A1C within the recommended range. However, managing diabetes is not without challenges. Because I often get hypoglycemic when hiking, I don't exercise as much as I may need for optimal health. The fear of hypoglycemia keeps me sitting at the computer. But that may soon change. A new type of insulin pump is on the market, and I have one of the first models, the Medtronic 670G. It's a closed-loop system. Readings from a CGMS are relayed back to the insulin pump, which can adjust insulin delivery to suit the need. On Tuesday, I was trained to set up and use the CGMS and 670G. There is a learning curve. I had my ACCU-Chek insulin pump and Dexcom CGMS for over four years. I had mastered the technology. I'll have to learn anew.





- Kunj Trivedi: Call of the Wild, 79, And Off To Chase A Cheetah, A Tryst With The Wild ↩
